Psychopathology of Frontal Lobe Syndromes
Michael H. Thimble, F.R.C.P., F.R.C. Psych
From Seminars in Neurology
Volume 10, No. 3
September 1990
Although personality and behavior disorders have been described following frontal lobe lesions since the mid part of the last century, it is remarkable how frontal lobe pathologic conditions often go unnoticed clinically, and indeed how the relevance of frontal lobe syndromes in man to an understanding of brain-behavior relationships has been neglected. This is in spite of the pertinent observations of Jacobsen (2) on the effects of frontal lobe lesions in primates, the careful reports of the consequences of head injuries in the World War II, (3) and of patients examined following prefrontal leukotomies, (4) all of which studies lead to the delineation of specific defects in behavior associated with lesions in this part of the brain. Their increasing significance and clinical relevance is noted by the recent publication of several monographs on frontal lobe syndromes (5,6) and the growing literature on various frontal lobe disorders, for example, frontal lobe dementias and frontal lobe epilepsies.
ANATOMIC CONSIDERATIONS
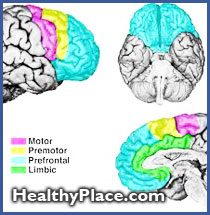
The frontal lobes are anatomically represented by those areas of the cortex anterior to the central sulcus, including the main cortical areas fur the control of motor behavior. The anterior cingulate gyrus can be considered part of the medial frontal lobe. The term "prefrontal cortex" is most appropriately used to designate the main cortical target projections for the mediodorsal nucleus of the thalamus, and this area is also sometimes referred to as frontal granular cortex. It is denoted by Brodmann areas 9-15, 46, and 47.
On the basis of primate data, Nauta and Domesick (7) suggested that the orbital frontal cortex makes connections with the amygdala and related subcortical structures and can be considered an integral part of the limbic system. Other important prefrontal connections are made by the mesocortical dopamine projections from the ventral tegmental area of the midbrain. Unlike subcortical dopamine projections, these neurons lack autoreceptors. (8) Further links from the frontal cortex are to the hypothalamus (the orbital frontal cortex alone in the neocortex projects to the hypothalamus), the hippocampus, and the retrosplenial and entorhinal cortices. It should further be noted that the prefrontal cortex sends projections to, but does not receive projections from, the striatum, notably the caudate nucleus, globus pallidus, putamen, and substantia nigra. A final point is that the area of the prefrontal cortex that receives the dominant dorsomedial thalamic nucleus overlaps with that from the dopaminergic ventral tegmental area.
From the neuropsychiatric point of view, therefore, the most relevant anatomic connections would appear to be frontothalamic, frontostriatal, frontolimbic, and frontocortical, the last deriving from the extensive reciprocal connections of the frontal lobes with sensory association areas, most notably the inferior parietal lobule and the anterior temporal cortex.
BEHAVIOR PROBLEMS WITH FRONTAL LOBE INJURY
 One of the specific behavior deficits following frontal lobe damage is attention disorder, patients showing distractibility and poor attention. They present with poor memory, sometimes referred to as "forgetting to remember." The thinking of patients with frontal lobe injury tends to be concrete, and they may show perseveration and stereotypy of their responses. The perseveration, with inability to switch from one line of thinking to another, leads to difficulties with arithmetic calculations, such as serial sevens or carryover subtraction.
One of the specific behavior deficits following frontal lobe damage is attention disorder, patients showing distractibility and poor attention. They present with poor memory, sometimes referred to as "forgetting to remember." The thinking of patients with frontal lobe injury tends to be concrete, and they may show perseveration and stereotypy of their responses. The perseveration, with inability to switch from one line of thinking to another, leads to difficulties with arithmetic calculations, such as serial sevens or carryover subtraction.
An aphasia is sometimes seen, but this is different from both Wernicke's and Broca's aphasia. Luria (9) referred to it as dynamic aphasia. Patients have well-preserved motor speech and no anomia. Repetition is intact, but they show difficulty in propositionizing, and active speech is severely disturbed. Luria suggested that this was due to a disturbance in the predictive function of speech, that which takes part in structuring sentences. The syndrome is similar to that form of aphasia referred to as transcortical motor aphasia. Benson (10) also discusses the "verbal dysdecorum" of some frontal lobe patients. Their language lacks coherence, their discourse is socially inappropriate and disinhibited, and they may confabulate.
Other features of frontal lobe syndromes include reduced activity, particularly a diminution of spontaneous activity, lack of drive, inability to plan ahead, and lack of concern. Sometimes associated with this are bouts of restless, aimless uncoordinated behavior. Affect may be disturbed. with apathy, emotional blunting, and the patient showing an indifference to the world around him. Clinically, this picture can resemble a major affective disorder with psychomotor retardation, while the indifference bears occasional similarity to the "belle indifference" noted sometimes with hysteria.
In contrast, on other occasions, euphoria and disinhibition are described. The euphoria is not that of a manic condition, having an empty quality to it. The disinhibition can lead to marked abnormalities of behavior, sometimes associated with outbursts of irritability and aggression. So-called witzelsucht has been described, in which patients show an inappropriate facetiousness and a tendency to pun.
Some authors have distinguished between lesions of the lateral frontal cortex, most closely linked to the motor structures of the brain, which lead to disturbances of movement and action with perseveration and inertia, and lesions of the orbital and medial areas. The latter are interlinked with limbic and reticular systems, damage to which leads to disinhibition and changes of affect. The terms "pseudodepressed" and "pseudopsychopathic" have been used to describe these two syndromes." A third syndrome, the medial frontal syndrome, is also noted, marked by akinesia, associated with mutism, gait disturbances, and incontinence. The features of these differing clinical pictures have been listed by Cummings, (12) as shown in Table I. In reality, clinically, most patients display a mixture of syndromes.
Table 1. Clinical Characteristics of the Three Principal Frontal Lobe Syndromes
Orbitofrontal syndrome (disinhibited)
Disinhibited, impulsive behavior (pseudopsychopathic)
Inappropriate jocular affect, euphoria
Emotional lability
Poor judgment and insight
Distractibility
Frontal convexity syndrome (apathetic)
Apathy (occasional brief angry or aggressive outbursts common)
Indifference
Psychomotor retardation
Motor perseveration and impersistence
Loss of self
Stimulus-bound behavior
Discrepant motor and verbal behavior
Motor programming deficits
- Three-step hand sequence
Alternating programs
Reciprocal programs
Rhythm tapping
Multiple loops
Poor word list generation
Poor abstraction and categorization
Segmented approach to visuospatial analysis
Medial frontal syndrome (akinetic)
Paucity of spontaneous movement and gesture
Sparse verbal output (repetition may be preserved)
Lower extremity weakness and loss of sensation
Incontinence
In some patients, paroxysmal behavior disorders are recorded. These tend to be short-lived, and may include episodes of confusion and, occasionally, hallucinations. They are thought to reflect transient disturbances of the frontolimbic connections. Following massive frontal lobe lesions, the so-called apathetico-akinetico-abulic syndrome may occur. Patients lie around, passive, unaroused, and unable to complete tasks or obey commands.
Further clinical signs associated with frontal lobe damage include sensory inattention in the contralateral sensory field, abnormalities of visual searching, echo phenomena, such as echolalia and echopraxia, confabulation, hyperphagia, and various changes of cognitive function. Lhermitte (13,14) has described utilization behavior and imitation behavior, variants of environmental dependency syndromes. These syndromes are elicited by offering patients objects of everyday use and observing that, without instruction, they will use them appropriately, but often out of context (for example, putting on a second pair of spectacles when one pair is already in place). They will also, without instruction, imitate an examiner's gestures, no matter how ridiculous.
EPILEPSY
The importance of making an accurate seizure diagnosis in patients with epilepsy has been accelerated in recent years by the use of advanced monitoring techniques such as videotelemetry. The more recent classification schemes of the International League Against Epilepsy recognize a major distinction between partial and generalized seizures (20) and between localization-related and generalized epilepsies. (21) In the latest classification (22) the localization-related epilepsies include frontal lobe epilepsies, in several different patterns. The general characteristics of these are shown in Table 2 and their subcategories in Table 3.
Table 2. International Classification of Epilepsies and Epileptic Syndromes
1. Localization-related (focal, local, partial) epilepsies and syndromes.
- 1.1 Idiopathic (with age-related onset)
1.2 Symptomatic
1.3 Cryptogenic
2. Generalized epilepsies and syndromes
- 2.1 Idiopathic (with age-related onset--listed in order of age)
2.2 Cryptogenic or symptomatic (in order of age)
2.3 Symptomatic
3. Epilepsies and syndromes undetermined as to whether they are focal or generalized.
Table 3. Localization-Related (Focal, Local, Partial) Epilepsies and Syndromes
1. 2 Symptomatic
- Chronic progressive epilepsia partialis continua of childhood (Kojewnikow's syndrome)
Syndromes characterized by seizures with specific modes of precipitation
Temporal lobe
Frontal lobe- Supplementary motor seizures
Cingulate
Anterior frontopolar region
Orbitofrontal
Dorsolateral
Opercular
Motor cortex
Parietal lobe
Occipital lobe - Supplementary motor seizures
They may be anatomically categorized, for example, into seizures arising from the rolandic area, the supplementary motor area (SMA). from polar areas (Brodmann areas 10, 11, 12, and 47), the dorsolateral area, the opercular area, the orbital region, and the cingulate gyrus. Rolandic seizures are typical jacksonian simple partial attacks, while SMA-derived attacks often lead to adversion with posturing and autonomic changes. Characteristic features of complex partial seizures arising from frontal areas include frequent clustering of brief seizures, with sudden onset and cessation. Often, the accompanying motor behavior may be bizarre; and, since the surface electroencephalogram (EEG) may be normal, these attacks may readily be diagnosed as hysterical pseudoseizures.
SCHIZOPHRENIA
That neurologic abnormalities underlie the clinical condition schizophrenia is now secure knowledge (see Hyde and Weinberger in this issue of Seminars). However, the precise pathologic lesions and the localization of the abnormalities continue to arouse interest and controversy. Much recent work has highlighted abnormalities of frontal lobe function in this condition. Several authors have drawn attention to the likeness of some schizophrenic symptoms to frontal lobe disorder, in particular that involving dorsolateral prefrontal cortex. Symptoms included are those of the affective changes, impaired motivation, poor insight. and other "defect symptoms." Evidence for frontal lobe dysfunction in schizophrenic patients has been noted in neuropathologic studies, (23) in EEG studies, (24) in radiologic studies using CT measures, (25) with MRI, (26) and in cerebral blood flow (CBF) studies. (27) The last have been replicated by findings of hypofrontality in several studies using positron emission tomography (PET). (28) These findings emphasize the importance of neurologic and neuropsychologic investigation of patients with schizophrenia, using methods that may uncover underlying frontal lobe disturbances, and the important role that frontal lobe dysfunction may play in the development of schizophrenic symptoms. (23)
DEMENTIA
The dementias are assuming increasing importance in psychiatric practice, and progress has been made with regard to classifying them and to discovering their underlying neuropathologic and neurochemical basis. While many forms of dementia involve frontal lobe changes, it is now clear that several types of dementia more selectively affect frontal lobe function, particularly early in the disease. The paradigm of frontal lobe dementia is that described by Pick in 1892, which was associated with circumscribed atrophy of both the frontal and temporal lobes. This form of dementia is much less common than Alzheimer's disease. It is more frequent in females. It may be inherited through a single autosomal dominant gene, although most cases are sporadic.
There are distinguishing features that reflect the underlying pathologic changes of Pick's disease and separate it from Alzheimer's disease. In particular, abnormalities of behavior, emotional changes, and aphasia are frequent presenting features. Some authors have noted elements of the Kluver-Bucy syndrome at one stage or another in the disease. (29) Interpersonal relationships deteriorate, insight is lost early, and the jocularity of frontal lobe damage may even suggest a manic picture. The aphasia is reflected in word-finding difficulties, empty, flat, nonfluent speech, and aphasia. With progression, the cognitive changes become apparent: these include memory disturbance but also impairment on frontal lobe tasks (see later). Ultimately, extrapyramidal signs, incontinence, and widespread cognitive decline are seen.
The EEG tends to remain normal in this disease, although CT or MRI will provide confirmatory evidence of lobar atrophy. The PET picture confirms diminished metabolism in frontal and temporal areas. Pathologically, the brunt of the changes is borne by these areas of the brain and mainly consists of neuron loss with gliosis. The characteristic change is the "balloon cell" which contains disordered neurofilaments and neurotubules, and Pick bodies, which are silver-staining and are also composed of neurofilaments and tubules.
Recently, Neary and colleagues (30) have drawn attention to a group of patients with non-Alzheimer's dementia who typically present with changes of personality and social conduct and with atypical Pick's changes in the brain. They note that this form of dementia may be more common than previously thought.
Another form of dementia that primarily affects frontal lobe function is that of normal pressure hydrocephalus. This may be related to several underlying causes, including cerebral trauma, previous meningitis, neoplasia, or subarachnoid hemorrhage, or it may occur idiopathically. Essentially, there is a communicating hydrocephalus with failure of absorption of cerebrospinal fluid (CSF) via the sagittal sinus through blockage, the CSF being unable to reach the convexity of the brain or be absorbed through the arachnoid villi. The characteristic clinical features of normal pressure hydrocephalus include gait disturbance and incontinence, with normal CSF pressure. The dementia is of recent onset and has characteristics of a subcortical dementia with psychomotor slowing and dilapidation of cognitive performance, in contrast to more discrete memory abnormalities that may herald the onset of Alzheimer's disease. Patients lose initiative and become apathetic; in some cases the presentation may resemble an affective disorder. In reality the clinical picture can be varied, but frontal lobe signs are a common feature and, especially when combined with incontinence and ataxia, should alert the physician to the possibility of this diagnosis.
Other causes of dementia that may present with an apparently focalized frontal picture include tumors, especially meningiomas, and rare conditions such as Kufs' disease and corticobasal degeneration.
DETECTION OF FRONTAL LOBE DAMAGE
Detection of frontal lobe damage can be difficult, especially if only traditional methods of neurologic testing are carried out. Indeed, this point cannot be overemphasized, since it reflects one of the main differences between traditional neurologic syndromes, which affect only elements of a person's behavior - for example, paralysis following destruction of the contralateral motor cortex -and limbic system disorders generally. In the latter it is the whole of the patient's motoric and psychic life that is influenced, and the behavior disturbance itself reflects the pathologic state. Often, changes can be discerned only with reference to the previous personality and behavior of that patient, and not with regard to standardized and validated behavioral norms based on population studies. A further complication is that these abnormal behaviors may fluctuate from one testing occasion to another. Therefore the standard neurologic examination will often be normal, as may the results of psychological tests such as the Wechsler Adult Intelligence Scale. Special techniques are required to examine frontal lobe function, and care finding out how the patient now behaves and how this compares with his premorbid performance.
Orbitofrontal lesions may be associated with anosmia, and the more the lesions extend posteriorly, the more neurologic signs such as aphasia (with dominant lesions), paralysis, grasp reflexes, and oculomotor abnormalities become apparent. Of the various tasks that can be used clinically to detect frontal pathologic conditions, those given in Table 4 are of value. However, not all patients with frontal damage show abnormalities on testing, and not all tests are found to be abnormal in frontal lobe pathologic states exclusively.
Table 4. Some Useful Tests at Frontal Lobe Function
Word fluency
Abstract thinking (if I have 18 books and two bookshelves, and I want twice as many books on one shelf as the other. how many books on each shelf?)
Proverb and metaphor interpretation
Wisconsin Card Sorting Test
Other sorting tasks
Block design
Maze lest
Hand position test (three-step hand sequence)
Copying tasks (multiple loops)
Rhythm tapping tasks
Cognitive tasks include the word fluency test, in which a patient is asked to generate, in 1 minute, as many words as possible beginning with a given letter. (The normal is around 15.)
Proverb or metaphor interpretation can be remarkably concrete.
Problem-solving, for example carry-over additions and subtractions, can be tested by a simple question (see Table 4). Patients with frontal lobe abnormalities often find serial sevens difficult to perform.
Laboratory-based tests of abstract reasoning include the Wisconsin Card Sort Test (WCST) and other object-sorting tasks. The subject must arrange a variety of objects into groups depending on one common abstract property, for example color. In the WCST, the patient is given a pack of cards with symbols on them that differ in form, color, and number. Four stimulus cards are available, and the patient has to place each response card in front of one of the four stimulus cards. The tester tells the patient if he is right or wrong, and the patient has to use that information to place the next card in front of the next stimulus card. The sorting is done arbitrarily into color, form, or number, and the patient's task is to shift the set from one type of stimulus response to another based on the information provided. Frontal patients cannot overcome previously established responses, and show a high frequency of preseverative errors. These deficits are more likely with lateral lesions of the dominant hemisphere.
Patients with frontal lobe lesions also do badly on maze learning tasks, the Stroop test, and block design; they show perseveration of motor tasks and difficulty carrying out sequences of motor actions. Skilled movements are no longer performed smoothly, and previously automated actions such as writing or playing a musical instrument are often impaired. Performance on tests such as following a succession of hand positions (with the hand first placed flat, then on one side, and then as a fist, on a flat surface) or tapping a complex rhythm (for example two loud and three soft beats) is impaired. Following nondominant hemisphere lesions, singing is poor, as is recognition of melody and emotional tone, the patient being aprosodic. Perseveration (especially prominent with deeper lesions in which the modulating function of the premotor cortex on the motor structures of the basal ganglia is lost (9) may be tested by asking the patient to draw, for example, a circle or to copy a complex diagram with recurring shapes in it that alternate one with another. The patient may continue to draw circle after circle, not stopping after one revolution, or miss the pattern of recurring shapes (Fig. 2). Imitation and utilization behavior can also be tested for.
In many of these tests there is a clear discrepancy between the patient's knowing what to do and being able to verbalize the instructions, and his failure to undertake the motor tasks. In everyday life this can be extremely deceptive and lead the unwary observer to consider the patient to be either unhelpful and obstructive or (for example, in a medicolegal setting) to be a malingerer.
Some of these tasks, for example the word-fluency task, or inability to make melodic patterns, are more likely to be related to lateralized dysfunction, and the inhibition of motoric tasks relates to the dorsolateral syndrome.
NEUROANATOMIC BASIS OF FRONTAL LOBE SYNDROMES
Several authors have put forward explanations for frontal lobe syndromes. (6,9) The posterolateral areas of the frontal cortex are most closely linked to motor structures of the anterior part of the brain, thus leading to the motor inertias and the perseverations seen with lesions here. They are more pronounced after dominant hemisphere lesions, when the speech-related disorders become manifest. More posterior lesions appear to link with difficulties in organizing movement; anterior lesions result in difficulties in motor planning and a dissociation between behavior and language. Elementary motor perseverations probably require lesions that are deep enough to involve the basal ganglia. Disturbances of attention are related to the brainstem-thalamic-frontal system, and the basal (orbital) syndromes are due to disruption of frontal-limbic links. Loss of inhibitory function over the parietal lobes, with release of their activity, increases the subject's dependence on external visual and tactile information, leading to echo phenomena and the environmental dependency syndrome.
Teuber (31) suggested that the frontal lobes "anticipate" sensory stimuli that result from behavior, thus preparing the brain for events about to occur. The expected results are compared with actual experience, and thus smooth regulation of activity results. More recently, Fuster (5) has proposed that the prefrontal cortex plays a role in the temporal structuring of behavior, synthesizing cognitive and motor acts into purposeful sequences. Stuss and Benson (6) put forward a hierarchical concept for the regulation of behavior by the frontal lobes. They referred to fixed functional systems, including a number of recognized neural activities, such as memory, language, emotion, and attention. which are modulated by "posterior" areas of the brain in contrast to the frontal cortex. Two anterior counterparts are proposed, namely, the ability of the frontal cortex to sequence, change set, and integrate information, and to modulate drive, motivation, and will (the former are most strongly dependent on intact lateral, dorsal and orbital frontal convexity regions; the latter are related more to medial frontal structures). A further independent level is that of executive function of the human frontal lobes (anticipation, goal selection, preplanning, monitoring), which is superordinate to drive and sequencing, but may be subordinate to the role of the prefrontal cortex in self-awareness.
SUMMARY
In this review, some basic aspects of frontal lobe functioning have been discussed and methods of testing for frontal lobe abnormalities outlined. It has been emphasized that the frontal lobes are affected in a number of diseases, which cover a broad spectrum of neuropsychiatric problems. Furthermore, it is suggested that the frontal lobes are involved in syndromes not traditionally thought to be related to frontal lobe dysfunction, for example, schizophrenia, and rarer presentations such as misidentification syndromes, Frontal lobe dysfunction often goes unrecognized, especially in patients who have normal neurologic testing and apparently intact IQ when routine methods of investigation are employed. Although marked disturbances of behavior following frontal lobe dysfunction have now been described for well over 120 years, these large areas of the human brain, and their links with some of the highest attributes of mankind, have been relatively neglected and are worthy of much further exploration by those interested in neuropsychiatric problems.
REFERENCES
1. Harlow JM. Recovery From the passage of an iron bar through the head. Publications of the Mass Med Soc 1898;2:129-46
2. Jacobsen CF. Functions and the frontal association cortex. Arch Neurol Psychiatry 1935;33:558-9
3. Weinstein S. Teuber ML. Effects of penetrating brain injury on intelligence test scores. Science. 1957;125:1036-7
4. Scoville WB. Selective cortical undercutting as a means of modifying and studying frontal lobe function in man: Preliminary report of 43 operative cases. J Neurosurg 1949;6:65-73
5. Fuster JM. The prefrontal cortex. New York: Raven Press, 1980
6. Stuss DT, Benson DF. The frontal lobes. New York: Raven Press. 1986
7. Nauta WJH, Domesick VB. Neural associations of the limbic system. In: Beckman A, ed. The neural basis of behavior. New York: Spectrum. 1982:175-206
8. Bannon CM, Reinhard JF, Bunney EB, Roth RH. Unique response to antipsychotic drugs is due to absence of terminal autoreceptors in mesocortical dopamine neurones. Nature 1982;296:444-6
9. Luria AR. The working brain. New York: Basic Books, 1973
10. Benson DF. Presentation to the World Congress of Neurology. New Delhi, India, 1989
11. Blumer D, Benson DF. Personality changes with frontal and temporal lobe lesions. In: Benson DF, Blumber D. eds. Psychiatric aspects of neurologic disease. New York: Grune & Stratton. 1975:151-69
12. Cummings JL. Clinical neuropsychiatry. New York: Grune & Stratton. 1985
13. Lhermitte F. Utilization behaviour and its relation to lesions of the frontal lobes. Brain 1983:106:237-55
14. Lhermitte F, Pillon B, Sedaru M. Human autonomy and the frontal lobes. Ann Neurol 1986:19:326-34
15. Mesulam M. Frontal cortex and behaviour. Ann Neurol 1986; 19:320-4
16. Pudenz RH, Sheldon CH. The lucite calvarium - a method of direct observation of the brain. J Neurosurg 1946:3:487-505
17. Lishman WA. Brain damage in relation to psychiatric disability after head injury. Br J Psychiatry 1968:114:373-410
18. Hillbom E. After effects of brain injuries. Acta Psychiatr Neurol Scand 1960;35(Suppl 142):1
19. Trimble MR. Post traumatic neurosis. Chichester: John Wiley & Sons. 1981
20. International League Against Epilepsy. Proposal for revised clinical and electroencephalographic classification of epileptic seizures. Epilepsia 1981:22:489-501
21. International League Against Epilepsy. Proposal for classification of the epilepsies and epileptic syndromes. Epilepsia 1985:26:268-78
22. International League Against Epilepsy. Proposal for revised classification of epilepsies and epileptic syndromes. Epilepsia 1989:30:289-99
23. Benes FM. Davidson J. Bird ED. Quantitative cytoarchitectural studies of the cerebral cortex of schizophrenics. Arch Gen Psychiatry 1986:43:31-5
24. Guenther W. Breitling D. Predominant sensory motor area left hemisphere dysfunction in schizophrenia measured by BEAM. Biol Psychiatry 1985:20:515-32
25. Golden CJ. Graber B, Coffman J. et al. Brain density deficits in chronic schizophrenia. Psychiatry Res 1980:3:179-84
26. Andreasen N. Nasrallah HA. Van Dunn V. et al. Structural abnormalities in the frontal system in schizophrenia. Arch Gen Psychiatry 1986:43:136-44
27. Weinberger DR. Berman KF. Zee DF. Physiologic dysfunction of dorsolateral prefrontal cortex in schizophrenia. Arch Gen Psychiatry 1986:43:114-24
28. Trimble MR. Biological psychiatry. Chichester: John Wiley & Sons. 1988
29. Cummings JL, Benson DF. Dementia, a clinical approach. London: Butterworths. 1983
30. Neary D. Snowden JS. Bowen DM. et al. Cerebral biopsy and the investigation of pre-senile dementia due to cerebral atrophy. J Neurol Neurosurg Psychiatry 1986:49:157-62
31. Teuber HL. The riddle of frontal lobe function in man. In: Warren JM, Akert K, eds. The frontal-granular cortex and behavior. New York: McGraw-Hill. 1964:410-44
next: Recommendations for Electroconvulsive Therapy (ECT) Consumer Guide
~ all Shocked! ECT articles
~ depression library articles
~ all articles on depression
APA Reference
Staff, H.
(2000, December 29). Psychopathology of Frontal Lobe Syndromes, HealthyPlace. Retrieved
on 2026, July 18 from https://www.healthyplace.com/depression/articles/psychopathology-of-frontal-lobe-syndromes